
















































CNA – Parents, check these eye-watering myopia stats: SNEC reports 65 per cent of Singaporean children aged 12 are myopic, and 83 per cent of young adults.
High myopia in children has doubled in a decade, now affecting up to 20 per cent. High myopia is a refraction of -6D or worse, explains Dr Janice Lam from NUH and Yong Loo Lin School of Medicine.
In simple terms, high myopia means 600 degrees or more. Some may have moderate myopia in one eye and high myopia in the other if there’s a difference between eyes.

Wondering why it matters? Glasses, contact lenses, or Lasik later can help, but myopia doesn’t always decrease as your child grows.
Here’s the lowdown: High myopia can lead to retinal detachment and if left untreated, permanent blindness. Your child also faces an increased risk of eye diseases at adulthood, including myopic macular degeneration, cataract and glaucoma, which can lead to vision impairment, said Dr Lam.
“Reducing myopia by 100 degrees has the potential to lower the risk of these eye conditions.”
There is help in the form of lifestyle tips and specialised contact lenses to stem the progress of myopia in young eyes. But first, let’s find out why myopia is so high among children here and what is retinal detachment in the first place.

WHY IS THE MYOPIA RATE IN CHILDREN SO HIGH IN SINGAPORE?
Blame the high myopia rates in kids on frequent near-work activities done on handheld gaming devices, personal computers, mobile phones and tablets, according to a Singapore Eye Research Institute study.
There’s also a genetic link, so having myopic parents can also increase a child’s risk. However, having to wear glasses has nothing to do with reading in dim lighting or sitting too close to the TV, the study found.
“Myopia can start at any age, although most children in Singapore are diagnosed with myopia at school health screenings in primary school,” said Dr Lam.
She has noticed that increasingly, children are becoming myopic at younger ages than before.
“In our eye clinic at NUH, patients are frequently referred to us with reduced visual acuity at their four-year-old developmental assessment.”

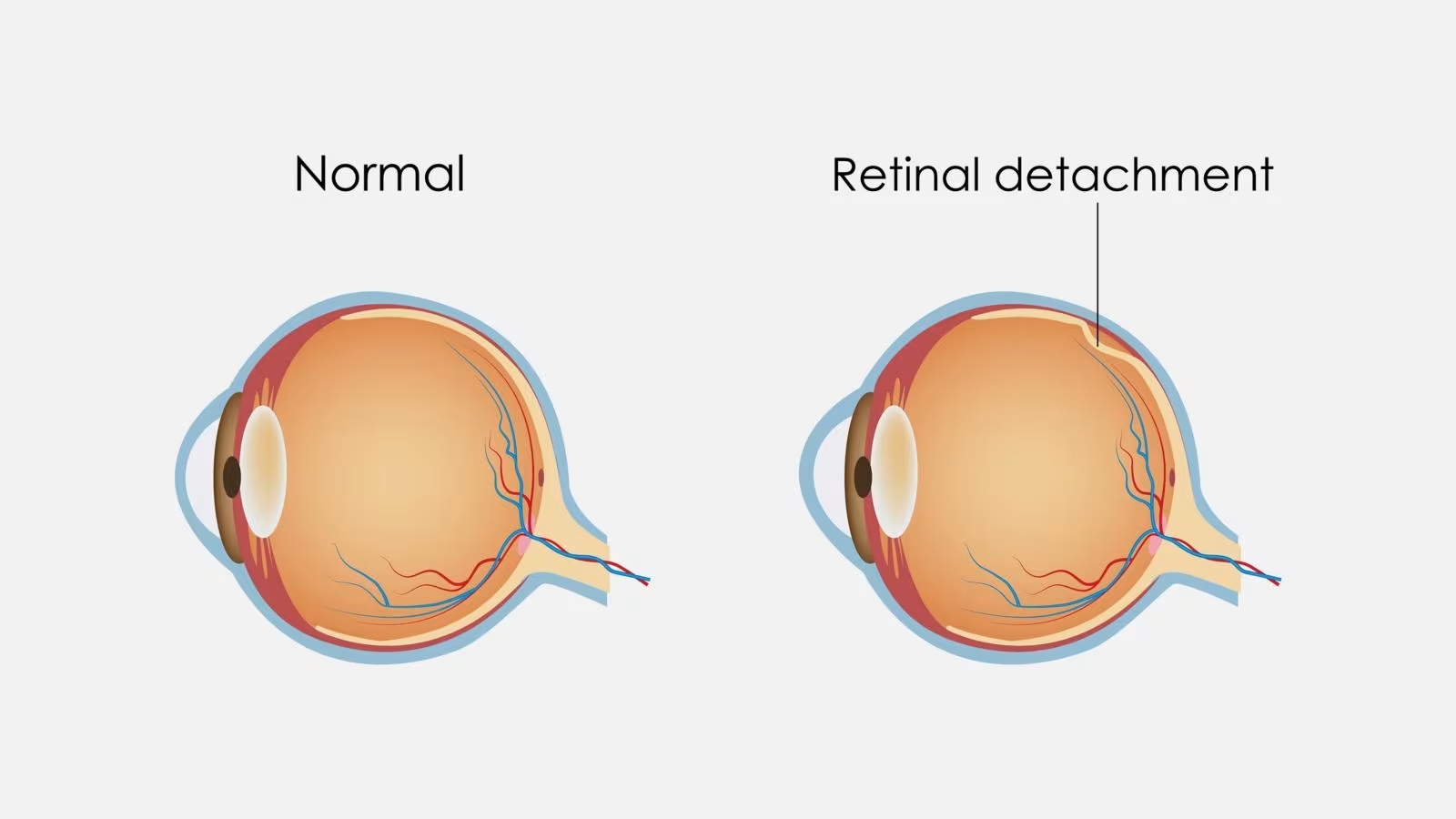
WHY DOES MYOPIA LEAD TO RETINAL DETACHMENT?
Think of the inside of your eyeball as an old-school cinema that uses a projector.
Normally, the projected movie should land squarely on the screen or in the eye’s case, the retina, to allow you to see things crisp and clear.
But in someone with myopia, the projector is moved further back, causing the image to hit the front instead of on the screen.
That extra room to move the projected image back comes from the elongation of the eyeball caused by myopia, explained Dr Lam, or what is known as an increase in axial length.
That’s not all. “Imagine the eye as a balloon and the retina as the skin of the balloon,” she said.
“The larger the balloon, the more the skin will stretch and thin out. There may come a point when the balloon is stretched beyond its limit and tears,” she said, creating retinal detachment.
DOESN’T MYOPIA IN CHILDREN USUALLY STABILISE OR EVEN REDUCE AS THEY GET OLDER?
Yes, most children and teenagers “will have a more stable refractive power by late adolescence to early adulthood”, said Dr Lam, “although I have seen some patients with progressive myopia into their early 20s”.
Myopia stabilises when the eye stops growing in length. “However, in some patients, myopia may continue to progress into adulthood due to various factors such as lifestyle habits, visual needs or eye conditions that cause the tissues of the eye to stretch and elongate,” said Dr Lam.
HOW SEVERE DOES THE MYOPIA HAVE TO BE TO CAUSE RETINAL DETACHMENT?
According to Dr Lam, there is no published incidence rate of retinal detachment in children with severe myopia in Singapore. However, “I have personally encountered a child with pathological myopia of 1,500 degrees, who developed a retinal detachment from her myopia”, she said.
Fortunately, most children in Singapore are usually found to have low to moderate myopia that ranges from below 200 degrees to 600 degrees, said Dr Lam.
WHAT ARE THE SIGNS THAT MY CHILD MAY HAVE RETINAL DETACHMENT?
Be on the alert if your child complains of seeing floaters, white flashes of light and/or having part of his vision obscured with a “black curtain” or loses his vision, said Dr Lam.
“If your child experiences any of these symptoms, seek emergency medical attention as soon as possible as permanent blindness can happen as quickly as a few days if left untreated, especially in the presence of a large retinal break,” she said.
CAN RETINAL DETACHMENT BE TREATED?
If the tears in the retina are picked up and treated in time, retinal detachment may be prevented, said Dr Lam. Depending on the extent of the detachment, the size and location of the retinal breaks, and the lens status of the eye, there are various surgical interventions available, including vitrectomy or scleral buckling, she said.
Dr Lam highlighted that post-operation, the child may be at risk of developing amblyopia or “lazy eye”, cataracts or glaucoma. “Hence, they must be regularly followed up with their ophthalmologist. However, there should not be any long-term restrictions to their lifestyle after retinal detachment surgery if the surgery was successful.”
IS THERE ANYTHING THAT CAN HELP BRING DOWN MY CHILD’S MYOPIA?
Getting your child to lay off the handheld gadgets would help, said Dr Lam. Other tips include taking frequent breaks when doing near-work such as reading.
Here’s one to try: After 20 minutes of near-work, let your child gaze at distant objects for 20 seconds or more. Don’t forget to let him spend time outdoors intermittently for at least two hours daily.
“Parents can consult their local paediatric ophthalmologist to enquire about the suitability of using low-dose atropine eye-drops in their children for the control of myopia,” suggested Dr Lam.
“Many randomised controlled trials conducted in Singapore and Hong Kong have established that low-dose atropine eye-drops are a safe and effective option in retarding myopia progression.”

I’VE HEARD ABOUT GLASSES AND CONTACT LENSES FOR CHILDREN THAT HELP TO REDUCE MYOPIA. HOW DO THEY WORK?
There are indeed spectacle lenses available in Singapore that can help to control myopia progression, said Dr Lam.
For instance, you can ask about the HALT (Highly Aspherical Lenslet Target) or DIMS (Defocus Incorporated Multiple Segments) lenses at your optician’s.
“These lenses have shown in clinical studies to help in controlling myopia by at least 50 per cent when compared with single vision lenses,” said Dr Lam.
If your child is active and glasses get in his way, there are daily disposable soft contact lenses available here such as MiSight 1 day to consider.
Each of these lenses has ring segments of higher power alternating with your child’s required power, explained Dr Ng Wei Yan, a consultant with SNEC’s Ophthalmology Department.
“The ring segments create areas of defocused light that land in the peripheral retina. When the eye senses these defocused areas, it creates a signal to reduce the rate of growth of the eyeball,” she said.
These lenses will have to be worn five or six days a week and eight to 10 hours a day.
Another type of contact lenses uses the process of orthokeratology or ortho-k to temporarily reshape the cornea with rigid contact lenses.
“As a result of the physical moulding, the shape of the cornea is changed temporarily to create these similar zones of defocus in the peripheral retina,” said Dr Ng.
“These lenses are often referred to as night lenses as they are worn at night to reshape the surface of the eye.”
Ortho-k lenses, also available at optical shops, are required to be worn for eight hours during sleep – and replaced every six to 12 months.
“When the myopia has stabilised during the teenage years, they can be switched to normal contact lenses or spectacles,” said Dr Ng. “This is usually after 15 years of age, where progression is usually minimal beyond that.”
HOW OLD MUST MY CHILD BE TO START USING CONTACT LENSES? HOW DO I KNOW IF MY CHILD IS SUITABLE?
From eight years old onwards if you’re considering letting your child try the soft contact lenses.
“Myopia control contact lenses are able to slow the elongation of the eye by approximately 50 per cent,” said Dr Ng.
The lenses can also work on older children, who have shown similar results as well, said Shila Gupta, Myopia Management General Manager the CooperVision Asia-Pacific.
For ortho-k lenses, research has shown that the ideal age to start is six years old. Primary and secondary school students also make good candidates as they experience the highest myopia progression, with an average increase of about 75 degrees per year.
The clear vision typically lasts about 18 hours after the rigid contact lenses are removed but can vary between 12 and 48 hours in some users.
Generally, children who have over 1,000 degrees in myopia or above 150 degrees in astigmatism are not suited for the daily soft contact lenses. Those with myopia of more than 600 degrees are not recommended for ortho-k lenses.
Other considerations include asking yourself: Is your child motivated enough to want to switch from glasses to contact lenses? Does he have the discipline to practise contact lens and hand hygiene?
If you’re uncertain, you can send your child to an optometrist to evaluate his ability to adapt. “Parents will need to be highly involved in the process, too, providing support and vigilant monitoring, while adhering closely to the treatment regime,” said Dr Ng.
“In cases where children may struggle with hygiene, daily replacement contact lenses are the preferred option since they can avoid contamination that may arise from the insufficient disinfection of contact lenses that are worn more than once,” said Shila. – Khoo Bee Khim

{kind=link}